Introduction
A) Display a normal large/small bowel, visually, and microscopically.

Above: Normal large bowel, visually (Nagasaki Univ.)

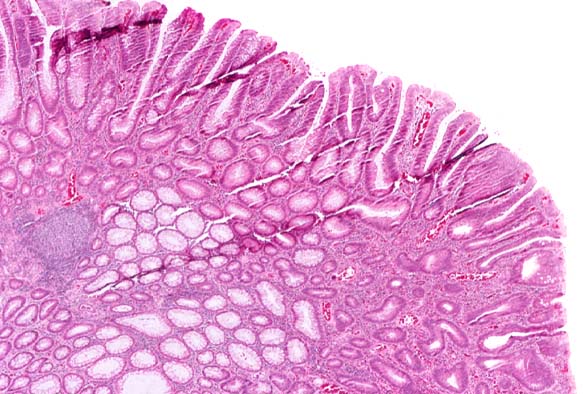
Above: Normal large bowel, microscopically (Loyola Univ.)

Above: Normal small bowel, visually (Univ. Iowa)

Above: Normal small bowel, microscopically (Pathnet UK)
B) Name its four layers, enumerate the types of cells in each layer, and name the types of possible benign and malignant proliferations possible from each of these cell types.
| LAYER | CELL TYPE | BENIGN PROLIFERATIONS | MALIGNANT PROLIFERATIONS |
| Mucosa | Simple Columnar Epithelium | | |
| | Enterocytes | | |
| | Goblet Cells | Adenomatous Polyp, Hyperplastic Polyp | Adenocarcinoma |
| | Paneth Cells | Adenomatous Polyp, Hyperplastic Polyp | Adenocarcinoma |
| | Enteroendocrine Cells | Adenomatous Polyp, Hyperplastic Polyp | Adenocarcinoma |
| | M Cells | | |
| | Lymphocytes | | |
| Submucosa | Brunner's Glands | Adenomatous Polyp, Hyperplastic Polyp | Adenocarcinoma |
| | Meissner's Plexus | | |
| Muscularis Propria | Smooth Muscle Cells | Leiomyoma | |
| | Auerbach's Plexus | | |
| Serosa | Simple Squamous Epithelium | | |
(Konishi, 1982)
C) Name the commonest malignant tumor, name at least two kinds of common benign tumors.
The most common type of malignant tumor is adenocarcinoma, and two types of common benign tumors are adenomatous and hyperplastic polyps. (Hassan, 2006)
Adenocarcinoma of the Colon
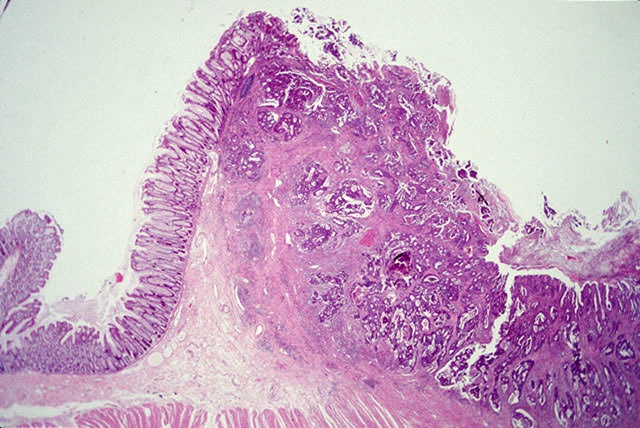
A) Define adenocarcinoma of the colon, show images at various microscopic powers. Show a side-by-side image comparing the malignant cells to their orderly cells of origin.
Adenocarcinoma of the colon is a malignant neoplastic epithelial lesion, arising from glandular tissue in the colonic mucosa. The cells do not necessarily need to be part of an existing gland, as long as they have secretory properties. Colonic adenocarcinomas often develop from previously benign colonic adenomas. These adenomas become adenocarcinomas as they transform into malignancies. (Kim, Brown Univ.)


The above images (low and high power magnification) show tumor cells deeply invading the mucosa layer of the colon. Glands will adhere together, and no longer display polarity. Cells in the epithelium show malignancy as they become hyperchromatic (darkly staining DNA), tightly packed, and contain a higher proportion of nucleus with respect to cytoplasm (Kim, Brown Univ.).

The image above (Dept. of Pathology, USUHS) shows a normal colonic epithelium. Compare with the image below (Dept. of Pathology, Johns Hopkins Univ.) of a colon with adenocarcinoma. These pictures clearly show how the normal glandular pattern becomes replaced with a chaotic appearance.
B) Define the various criteria which make the tumor malignant or benign. Describe all of the tumor cells and the cells reacting to it.
A benign tumor is an adenoma, while the malignant type is described as adenocarcinoma. The following biological criteria of cells determine the tumor's status:
-Benign cells will be well-differentiated, and malignant cells may be undifferentiated
-Benign cells wil display limited and slow growth, and malignant cells will be unrestricted and often rapid in growth
-Benign cells are non-invasive and non-metastatic, and malignant cells are invasive and metastatic
-Benign cells have a uniform shape, and malignant cells are varied in shape
(Robbins, 1999)
Cells which are part of the origin of the tumor are glandular in nature. This includes goblet cells, Paneth cells, enteroendocrine cells, and Brunner's glands. The cells which react are enterocytes, M cells, lymphocytes, and possibly serosal epithelium and smooth muscle cells of the muscularis propria layer.
(Sinauer Assoc. Publishers)
C) Define the main histologic criteria making the tumor malignant or benign.
Histologically, adenomas and adenocarcinomas originate in the glandular portion of epithelial tissue. For a tumor to be malignant, the following histology is identified:
-Malignant cells have a higher nuclear to cytoplasmic (N/C) ratio than benign cells
-Malignant cells appear disorganized in comparison to benign cells
-Malignant cells are often more hyperchromatic (DNA stains more darkly) than benign cells
(Robbins, 1999)
D) In your own words, describe the causative factors for the tumor.
There are many risk factors associated with an adenocarcinoma but the majority of adenocarcinomas come from a preexisting adenoma that may be villous or tubular. The other causative factor is from dysplasia which is a premalignent condition within the flat mucosa (25). Patients with and adenomatous polyposis syndromes like familial polyposis which is where a mutant APC tumor suppressor gene is inherited, or hereditary nonpolyposis colorectal cancer syndromes which is where a mutation in DNA mismatch repair genes are inherited are more prone to acquire adenocarcinomas (27).
E) In your own words, describe the main clinical symptoms, if any.
Hidden (occult) and chronic rectal bleeding is the main clinical symptom of an adenocarcinoma and it may reveal itself as an iron deficient anemia. Many may attribute this rectal bleeding to hemorrhoids but should get it examined. Patient may feel fatigued and look pale. If the adenocarcinoma is large it may obstruct the colon and patient may get distention in the abdomen without any weight gain, narrow ribbon-like stool, inexplicable nausea or vomiting, weight loss, change in bowel movements, and the feeling of remaining stool after a bowel movement. Rarely does a patient have rectal or abdominal pain (26,27).
F) In your own words, describe various radiologic methods of detection, if any.
A barium enema x-ray is used to detect larger (greater than 1 cm) adenocarcinomas. It is an excellent method that is also cost effective. Liquid with barium is introduced into the rectum or anus and detect adenocarcinomas. However, a colonoscopy allows the doctor to actually remove any polyps and send them to be biopsied.
G) In your own words, describe various lab test to aid diagnosis, if any.
There are no real lab tests to diagnose adenocarcinomas. There is a fecal occult blood test to determine if there is indeed blood in a patient's stool. A close eye on carcinoembryogenic antigen (CEA) can help detect a recurrence. Upon colonoscopy and biopsy of a mass, histologically it can be determined if the mass is an adenocarcinoma.
H) In your own words, describe the biologic behavior of this tumor, particularly with respect to grading and staging. Define grading, define staging, in your own words. Define the Dukes staging criteria.
Determining how quickly and how aggressively a tumor is growing one has determined its GRADE. The STAGE of the tumor, however, determines how far it has spread within the body. The Dukes’ staging criteria is an older classification scheme that was used to help determine the development of the mass and how involved it was within the tissue. That scheme has now been replaced according to the National Cancer Institute by the TNM (Tumor, Node, Metastasis) system which is more specific and detailed in order to best assist determining treatment and prognosis.
Based on the TNM system of classification which is the one that is currently used, the tumor begins to invade more and more layers of the colon and this biological behavior is what determines the increase in its grading. As more and more lymph nodes become engaged, the classification also increases. Then there are many combinations of the classifications that give an overall stage of the adenocarcinoma. This is all defined below in the TNM system.
The Dukes staging criteria is as follows. There are stages A-D and they are defined as:
Dukes Stage A: A carcinoma in situ limited to mucosa or submucosa
Dukes Stage B: Cancer that extends into the muscularis, into or through the serosa
Dukes Stage C: Cancer that extends to regional lymph nodes
Dukes Stage D: Cancer that has metastasized to distant sites
Now the TNM system looks as follows according to the National Cancer Institute site.
The tumor, node, and metastasis are each given a classification and then the staging is determined from there according to the American Joint Committee on Cancer (AJCC):
Primary tumor (T)
• TX: Primary tumor cannot be assessed
• T0: No evidence of primary tumor
• Tis: Carcinoma in situ: intraepithelial or invasion of the lamina propria
• T1: Tumor invades submucosa
• T2: Tumor invades muscularis propria
• T3: Tumor invades through the muscularis propria into the subserosa or into nonperitonealized pericolic or perirectal tissues
• T4: Tumor directly invades other organs or structures and/or perforates visceral peritoneum
Regional lymph nodes (N)
• NX: Regional nodes cannot be assessed
• N0: No regional lymph node metastasis
• N1: Metastasis in 1 to 3 regional lymph nodes
• N2: Metastasis in 4 or more regional lymph nodes
Distant metastasis (M)
• MX: Distant metastasis cannot be assessed
• M0: No distant metastasis
• M1: Distant metastasis
AJCC stage groupings
Stage 0: Tis, N0, M0
Stage I: T1, N0, M0 OR T2, N0, M0
Stage IIA: T3, N0, M0
Stage IIB: T4, N0, M0
Stage IIIA: T1, N1, M0 OR T2, N1, M0
Stage IIIB: T3, N1, M0 OR T4, N1, M0
Stage IIIC: Any T, N2, M0
Stage IV: Any T, Any N, M1
I) In your own words, describe the management of this tumor, with respect to its biologic behavior, i.e., extent.
If the number of polyps is small then excision is recommended upon colonoscopy. However, if it is a large amount and well developed then it is best to surgically remove that portion of the colon and follow it up with chemotherapy if it has spread to the lymph nodes. Radiation is also helpful before surgery in order to reduce the size of the tumor and helps with reducing recurrence. Close monitor after surgery and watching CEA levels helps in detecting recurrence. Sometimes the tumor is so large that a permanent colostomy is created upon removal of the tumor. Managing the tumor all depends on where and how large the tumor is. (25, 26)
Hyperplastic Polyps
A) Define hyperplastic polyps of the colon, show images at various microscopic powers. Show a side-by-side image comparing the malignant cells to their orderly cells of origin.
A hyperplastic polyp of the colon is a polyp that is benign and does not possess a threat to becoming cancerous. They are the most common and have normal cellular components. They can be small and nodular or polypoid. They do not display dysplasia.

This is an image of a sessile or flat hyperplastic colon polyp (left) and an adenomatous polyp on the right. Note that they cannot really be told apart visually.


The above images are that of hyperplastic polyps of the colon taken from www.pathology.pitt.edu/lectures/gi/colon-a/14.htm.
Above is an image of a hyperplastic polyp at mag 40X. (28)

Above is an image of a hyperplastic polyp at mag 100X. (28)
Below are side by side images of a normal colon (left) and one with a hyperplastic polyp (right). These images were taken from patients.uptodate.com


Note the difference in the crypts and the serrated surface in the hyperplastic polyps.
B) Define the various criteria which make the tumor malignant or benign. Describe all of the tumor cells and the cells reacting to it.
Hyperplastic polyps are the most common type of polyp found in the colon. The term ‘hyperplastic’ refers to an increase in the number of cells, although, they are usually benign lesions less than 1/4 inch in diameter. Hyperplastic polyps are most often found in the descending colon and rectum of elderly patients.
Upon examination, hyperplastic polyps can be described as rice grains on the colonic mucosa, with minimal epithelial atypia (8). An abnormality in the cellular replication mechanism can result in the proliferation of cells in colonic crypts. The cells of hyperplastic polyps display normal differentiation and maturation. In the lower part of the crypt, cells become more crowded and hyperchromatic (10). The scalloped appearance of the mucosa is imparted by the variable height of hyperplastic goblet cells located in the upper part of the crypts (4,8). Formation of the hyperplastic polyp is ultimately due to the absence of shedding of mature cells into the intestinal lumen.
C) Define the main histologic criteria making the tumor malignant or benign.
Histologically, hyperplastic polyps still maintain generalized tissue organization and normal differentiation of cell types. Hyperplastic polyps are benign in that they lack the potential to spread to other tissue and once diagnosed, no further follow-up examination is required (6). Careful examination of polyp biopsies is important in differentiating benign and malignant lesions. In some instances, hyperplastic polyps may present with misplaced epithelium, mimicking the characteristics of an adenoma. Admixed polyps and serrated adenomas have characteristics intermediate to benign and neoplastic lesions. Serrated adenomas have highly mitotically active L-shaped glands that make them premalignant (4,8).
D) In your own words, describe the causative factors for the tumor.
Some data has shown an increased presence of hyperplastic polyps with age, low folate intake, alcohol consumption, and current cigarette smoking (4). The incidence of hyperplastic polyps also seems to have a genetic component, where DNA methylation patterns can predict the progression to malignancy in patients with hyperplastic polyposis syndrome (9).
E) In your own words, describe the main clinical symptoms, if any.
Usually, there are no clinical symptoms associated with the presence of hyperplastic polyps. They are usually found upon screening or diagnostic testing of the colon through flexible sigmoidoscopy or complete colonoscopy (4). However, they can occasionally cause rectal bleeding and rarely partial bowel obstruction if large enough (6).
F) In your own words, describe various radiologic methods of detection, if any.
Flexible sigmoidoscopy and complete colonoscopy are the preferred methods of polyp detection. However, single contrast barium enema can be sufficient for detecting polyps, if either sigmoidoscopy or colonoscopy are not possible. The radiologic method of detection has limitations in that it does not allow for biopsy or polypectomy of the lesion (6). Virtual colonoscopy may be performed if traditional endoscopic methods are not an option. Flat or sessile polyps have a greater chance of being missed with this type of detection method (5). In all cases, the type of polyp, either neoplastic or non-neoplastic can only be determined by histological methods.
G) In your own words, describe various lab test to aid diagnosis, if any.
The primary method of diagnosing hyperplastic polyps is careful pathological examination of polyp biopsies taken during sigmoidoscopy or total colonoscopy. Histological staining can demonstrate the hyperchromaticity of the lower portions of crypts. No other laboratory tests have been mentioned.
H) In your own words, describe the biologic behavior of this tumor, particularly with respect to grading and staging. Define grading, define staging, in your own words. Define the Dukes staging criteria.
Hyperplastic polyps, in general, are not considered cancerous or precancerous and thus there is no specific staging or grading associated with polyps. However some forms of colorectal cancer develop slowly over several years and usually begin as a polyp i.e. does not start out as a cancer but may eventually change into one. Thus hyperplastic polyps might be a sign that the person is likely to develop adenomatous polyps and cancer.
Grading:
Grading as it applies to tumors is a measure of its progress or of the gegree of differentiation of a cell type. A tumor or cancerous growth is often attributed to a lack of differentiation of the cell types. Thus an important part of evaluating a cancer is to determine how differentiated a cell is i.e. the extent to which cancer cells are similar in appearance and function to healthy cells of the same tissue type.
Staging:
Staging is the process of defining the degree of advancement of the specific type of malignancy in the patient at the time of presentation (i.e. the time when the diagnosis is made). The organ and cell type in which the malignancy has developed defines the type of malignancy.
Dukes staging criteria:
Dukes' staging is a pathological staging based on resection of the tumor and measures the depth of invasion through the mucosa and bowel wall. It does not take into account the level of nodal involvement nor the grade of the tumor.Dukes staging consists of 4 sub-levels (A trough D).A --> Confined to mucosaB --> Varies by system (Confined to muscularis)C --> Positive lymph nodesD --> Distant metastases
I) In your own words, describe the management of this tumor, with respect to its biologic behavior, i.e., extent.
Hyperplastic polyps are not thought to carry a malignant potential. However it would be reasonable to treat these in a manner analogous to that of adenomatous polyps. Because Hyperplastic polyps may be indistinguishable grossly from adenomatous polyps
One of multiple Hyperplastic polyps should be excised to confirm the true nature of the lesion. Attempts to remove the polyps should be made. If the colon can be cleared, then it can be reasonably assured that there is no evidence of dysplasia. If the polyps cannot be completely removed due to size or number, then consideration of more frequent surveillance is warranted.
Adenomatous Polyps
A) Define adenomatous polyps of the colon, show images at various microscopic powers. Show a side-by-side image comparing the malignant cells to their orderly cells of origin.

Adenomatous polyp
Adenomatous polyp is a benign neoplastic growth with variable malignant potential. It is visible as protrusions that can develop on the mucosal surface of the colon or the rectum

Normal Colon

Colon with multiple Adenomatous polyps

Adenomatous Polyp 10X (28)

Junction of non-neoplastic and adenomatous epithelium 100X (28)

Adenomatous epithelium 400X (28)
B) Define the various criteria which make the tumor malignant or benign. Describe all of the tumor cells and the cells reacting to it.
All adenomas have variable degrees of dysplasia ranging from low-grade to high-grade. Classically, it is believed that the malignant potential of adenomas correlates with type of polyp, size, and degree of dysplasia. Higher grades of dysplasia, increasing percentage of villous tissue within the polyp, and polyps greater than 1 cm in diameter are associated with increased risk of malignancy. A polyp is considered malignant when cancer cells within the neoplasm have extended to the submucosa via penetration through the muscularis mucosal layer.
C) Define the main histologic criteria making the tumor malignant or benign.
All adenomatous polyps are dysplastic, by definition, exhibiting abnormal histology with hypercellularity, loss of zonal proliferation, appearance of some cellular heterogeneity, hyperchromatic nuclei and basophilic cytoplasm.
The earliest appearance of malignant cells in an adenomatous polyp may be difficult to ascertain. Initially, highly dysplastic cells (i.e. cells with extreme nuclear atypia and pleomorphism, increased nuclear-cytoplasmic ratio and stratification) may still be confined to the epithelial surface layer, a state known as intraepithelial carcinoma at this stage the polyp might still be benign. A more reliable and advanced sign of malignant behavior is the invasion of the atypical epithelial cells through the basement membrane and into the submucosa.
D) In your own words, describe the causative factors for the tumor.
Adenomatous polyps are common and do not have a single significant causative factor. Patients may have more than one polyp, and the risk of having polyps increases with age. The chance of having polyps is also increased with a family history of colorectal polyps or colorectal cancer, including inherited disorders such as Gardner’s syndrome or familial adenomatous polyposis. As is consistent with other forms of cancer exposure to certain methylating agents can also increase the risk of adenomatous polyps.
E) In your own words, describe the main clinical symptoms, if any.
Most adenomas are asymptomatic until they grow to 2cm or more in diameter. The most common symptom however is rectal bleeding, mucous discharge or prolapse. If a polyp is large enough, it can simulate faeces so the colon undergoes vigorous muscular movements or peristalsis in a futile attempt to expel the polyp. This can lead to severe colicky pains.
F) In your own words, describe various radiologic methods of detection, if any.
Most polyps are discovered at the time of colon cancer screening. One preferred method is the flexible sigmoidoscopy, which can detect adenomatous polyps in the sigmoid. If found, a full colonoscopy is required for detection and removal of other polyps higher in the colon. An older method is the barium enema, which can detect polyps with an xray. There are efforts presently to develop a radiologic colonoscopic test, a virtual colonoscopy, where a CAT scan is used to detect the presence of polyps in the colon. The role of this screening technique is limited to simply screening populations at lower risk for polyps and may not pick up smaller polyps. However, the technique is continually improving.
G) In your own words, describe various lab test to aid diagnosis, if any.
Before the colonoscopy, a physician can take a stool sample and check for occult blood in the lab. Large polyps can bleed into the intestine where the blood mixes with the stool. This can be a sign of adenomatous polyps. In the works are blood tests which look at genetic predisposition to polyps. After a colonoscopy, a polyp can be sent to the lab for a biopsy to see if it is adenomatous. Under the microscope, further classification of the polyp as either tubular, villous, or tubulo-villous can help diagnosis. Villous polyps are the most likely to become cancerious, while tubular ones are the least.
H) In your own words, describe the biologic behavior of this tumor, particularly with respect to grading and staging. Define grading, define staging, in your own words. Define the Dukes staging criteria.
Adenomatous polyps are neoplastic and direct precursors to adenocarcinoma, but are not yet cancerous cells and so are not graded and staged until they develop into cancer. Once cancerous, they can be graded and staged. The grading of a cancer is a measurement of the cancer cell’s aggressiveness or rate of growth. It can be measured on a 2-10 scale (or 1-3 for breast cancer): cancer cells that look like normal cells with some aggressiveness (level 4), intermediate levels (5-7), really aggressive cells (8-10). The staging of the cancer is a measurement of the cancer’s extent of growth to other parts of the body. The cancer starts at the epithelial mucosa and can grow into the muscularis mucosa (level 1 tumor), the submucosa (level 2), the muscularis propria (level 3), and finally through the serosa and into other organs (level 4). Similar classifications can be used to describe the number of lymph nodes and level of metastases. Dukes staging criteria is similar and measured with A-D: Tumor is found only in the surface of intestinal wall (A), tumor invades into the wall (B), lymph nodes are involved (C), and metastasis (D).
I) In your own words, describe the management of this tumor, with respect to its biologic behavior, i.e., extent.
In order to manage the behavior of adenomatous polyps, any detected polyps necessitate the use of a full colonoscopy in order to detect and remove other polyps higher in the colon. This reduces the chances of adenomatous polyps growing into cancerous tumors. Additional colonoscopies usually follow, with a recommendation of a colonoscopy every 5 years or 3 years after removal of more dangerous polyps. Polyps can be fairly common, especially as people age. They typically don’t cause many symptoms, with painless rectal bleeding the most common. It is estimated that 50% of the people over the age of 60 will have atleast one polyp. The larger these polyps become, the more likely the risk of cancer. When it is 2 cm, the chance of it becoming cancerous is 20%. If there are multiple polyps, a surgical consultation is usually required.
Leiomyoma of the Muscularis
A) Define leiomyoma of the muscularis of either small or large bowel, show images at various microscopic powers. Show a side-by-side image comparing the malignant cells to their orderly cells of origin.
The definition of Leiomyoma is a cancer of the smooth muscle. Although most gastrointestinal leiomyomas occur in the stomach, it can also occur in the colon, specifically in the muscularis layer. However, leiomyoma of the colon is rare. According to Modern Pathology (USCAP), “the small number of reported cases does not allow for clinicopathologic profiling.” Endoscopically, they may look like pedunculated intramural or intraluminal polyps and usual adenomas and The Internet Journal of Surgery (ISPUB.com) says that they should be considered a differential diagnosis on encountering a polyp during endoscopic exams.
An Asterisk marks the muscularis layer of the normal colon.

High Magnification of Smooth Muscle Cells in Leiomyoma. Note the elongated spindle cells containing cigar-shaped nuclei and no mitotic activity.

B) Define the various criteria which make the tumor malignant or benign. Describe all of the tumor cells and the cells reacting to it.
Smooth muscle tumors can be benign or malignant. The Internet Journal of Surgery suggests that the behavior of the tumor cannot simply be determined by histological analysis because benign-looking cells are still metastatic. It is suggested that “a combination of the site, tumor size, histological appearance and mitotic count gives the best predictor of behavior.”
Conversely, the general consensus seems to state that leiomyomas are all benign. Modern Pathology (USCAP) describes the tumors best:
“All tumors were composed of well-differentiated, eosinophilic smooth muscle cells that were seen immediately beneath the mucosa obliterating the muscularis mucosae layer and merging with it. Two tumors had significant atypia ("symplastic leiomyoma"); mitotic activity was seen in one of these tumors, but not in others. The lesional cells were uniformly positive for smooth muscle actin and desmin and negative for CD34, CD117 and S100-protein, based on immunohistochemical studies on 20 to 24 cases with each marker.”
C) Define the main histologic criteria making the tumor malignant or benign.
Histologically, intestinal leiomyoma can be differentiated from leiomyosarcoma, because despite the fact that both have increased cellularity, leiomyomas have less mitotically active nuclei. Less than 2 mitotically active nuclei per hpf is considered benign. See the light micrographs below to compare leiomyomas and leiomyosarcomas (20).

Leiomyoma 1 (medium power)

Leiomyoma 2 (high power)

Leiomyosarcoma 1 (low power)

Leiomyosarcoma 2 (medium power)

Leiomyosarcoma 3 (high power)
D) In your own words, describe the causative factors for the tumor.
The causative factors of intestinal leiomyomas are unknown (19).
E) In your own words, describe the main clinical symptoms, if any.
Major clinical symptoms of intestinal leiomyoma vary with the size of the tumor. Smaller tumors are asymptomatic and are only discovered when medical investigation of other problems leads to their discovery (i.e. laparotomy, autopsy, radiological examinations). Larger tumors lead to bowel obstruction and bleeding (19).
F) In your own words, describe various radiologic methods of detection, if any.
To detect these tumors capsule endoscopy is used. This procedure involves a small capsule sized camera that is lead through the intestine in order to view the lumen of the bowels (19).
G) In your own words, describe various lab test to aid diagnosis, if any.
Lab tests are not usually performed. The best diagnostic methods are radiologic (19).
H) In your own words, describe the biologic behavior of this tumor, particularly with respect to grading and staging. Define grading, define staging, in your own words. Define the Dukes staging criteria.
Intestinal leiomyomas are classified as a 2.2 according to the World Health Organization Histologic Classification of Tumors of the Colon and Rectum. Category 2 tumors are non-epithelial (i.e. lipomas, leiomyomas, gastrointestinal stromal tumors, etc.) (22).
The term staging is used when a physician has diagnosed that a patient has a malignant tumor and at what period is it in. In short, staging tells the level of malignant cells present. The term grading is used to describe how malignant a cell is, this is with respect to a normal cell. Grade is determined via microscopic investigation and can range from low grade to high grade (21).
The Dukes staging system consists of 4 categories (A-D). Each is characterized as:
A.The tumor made its way only as deep as the mucosa.
B1.The tumor made its way to the muscularis propria.
B2.The tumor made its way through the muscularis propria.
C1.The tumor made its way to the muscularis propria and there is now cancer to the lymph nodes.
C2.The tumor made its way through the muscularis propria and there is now cancer to the lymph nodes.
D.The tumor made its way beyond the intestine and has begun to spread to nearby organs (23).
I) In your own words, describe the management of this tumor, with respect to its biologic behavior, i.e., extent.
Leiomyomas are handled with great care so that all tumors can be found with success. Various forms of endoscopy (i.e. capsule, enteroscopy, etc) are used to determine size and location of the tumors.The tumors are viewed and removed by laparotomy, as well as segemental resection in extreme cases. Removal of these benign tumors is usually successful (19).
Group members
- Iris Corbin
- Soleil Leilabadi
- Christine Mata
- Amanpreet Sherwal
- Sinh Tran
- Kimberly Zamor
Sources
- Kim, John P., M.D., http://www.brown.edu/Courses/Digital_Path/GI/colonic_adenocarcinoma.htm
- Dept. of Pathology, Uniformed Services University of the Health Sciences, http://www.usuhs.mil/pat/surg_path/nlhist/pictures/nl0038.jpg
- Dept. of Pathology, Johns Hopkins University, http://oac.med.jhmi.edu/pathconcepts/ShowImage.cfm?TutorialID=9&ConceptID=53&ImageID=236
- The Doctor’s Doctor, http://www.thedoctorsdoctor.com/diseases/gi_hyperplastic_polyp.htm
- Pathology Associates of Lexington, PA, http://www.palpath.com/MedicalTestPages/polypcol.htm
- Bond, John H., M.D., http://www.acg.gi.org/physicians/guidelines/NonfamilialColorectalPolyps.pdf
- Virtual Slidebox of Histopathology, Univeristy of Iowa, http://www.path.uiowa.edu/virtualslidebox/iowa_histopathology/content_index_db.html
- Friedlander, Ed, M.D., Pathologist, http://www.pathguy.com/lectures/guts.htm
- Enders, Gregory H., M.D., PhD, http://www.emedicine.com/med/topic414.htm
- Varma, Jay R., and Luther R. Mills, http://findarticles.com/p/articles/mi_m0689/is_n2_v35/ai_12591847
- Nagasaki Univ., Dept. of Pathology, http://www-sdc.med.nagasaki-u.ac.jp/n50/disaster/Colon-E.html
- Loyola Univ. School of Medicine, http://www.meddean.luc.edu/lumen/MedEd/Pathology/images/gi43.jpg
- Univ. of Iowa Dept. of Pediatrics, http://www.uihealthcare.com/topics/medicaldepartments/pediatrics/organmap/smbowel.html
- Pathnet UK, http://www.pathnet.org.uk/moodle/file.php/1/Tapir_Links/Normal_Small_Bowel-5526-6297.jpg
- Konishi, et al, Journal of Clinical Pathology, 1982;35:830-841
- Sinauer Associates, Inc publishers, http://www.sinauer.com/pdf/nsp-cellcycle-12-2.pdf
- Hassan, et al 2006, http://www.emedicine.com/radio/topic182.htm
- Robbins- Pathologic Basis of Disease, 6th edition. eds. W.B.Saunders Company, Philadelphia, PA, 1999.
- Terry, Shawn M., and Thomas Santora. "Benign Neoplasm of the Small Intestine." EMedicine. 27 Dec. 2006. Penn State University. 28 Dec. 2006 <http://www.emedicine.com/med/topic2652.htm>.
- "Pathology Review." Neoplasia. University of Texas Houston. 28 Dec. 2006 <http://medic.med.uth.tmc.edu/edprog/Path/Neo1/NeoI.htm>.
- "Tumor Staging." ENotes.Com. 2007. 2 Jan. 2007 <http://health.enotes.com/cancer-encyclopedia/tumor-staging>.
- "Human Colorectal Cancer." National Cancer Institute. U.S. National Insititute of Health. 2 Jan. 2007 <http://emice.nci.nih.gov/emice/mouse_models/organ_models/gastro_models/human_colorectal_cancer/>
- "Colorectal Cancer." Oncology Channel. 28 Sept. 2006. HealthCommunities.com. 2 Jan. 2007 <http://www.oncologychannel.com/coloncancer/staging.shtml>.
- Philomena M. Colucci, DO, MS, Steven H. Yale, MD, and Christopher J. Rall, MD "Colorectal Polyps" PubMed <http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1069054>
- Buetow, Peter, James L. Buck, Norman J. Carr, and Linda Pantongrag-Brown. Colorectal Adenocarcinoma. RadioGraphics. January 1, 1995 Vol 15, Number 1. http://www.rsna.org/REG/publications/rg/afip/privateM/1995/0015/0001/0127/1.htm#topAnchor
- http://www.emedicinehealth.com/colon_cancer/article_em.htm
- Wafik S El-Deiry, MD, PhD. Colon Cancer, Adenocarcinoma. http://www.emedicine.com/MED/topic413.htm
- Pathology Education Resources Laboratory of the Department of Pathology at Indiana University School of Medicine <http://erl.pathology.iupui.edu/>
- Miettinen M.D., Sarlomo-Rikala M.D. and Sobin M.D., http://www.nature.com/modpathol/journal/v14/n10/full/3880417a.html
- N. Husain, R. Botchu, M.M. Shahabdeen, J. Schofield, L.M. South: Leiomyoma Of The Rectosigmoid Junction In An Adult. The Internet Journal of Surgery. 2005. Volume 7 Number 1. http://www.ispub.com/ostia/index.php?xmlFilePath=journals/ijs/vol7n1/leiomyoma.xml#e1
- National Cancer Institute website. http://www.cancer.gov/cancertopics/pdq/treatment/colon/HealthProfessional/page1
- http://patients.uptodate.com/image.asp?file=gast_pix/hyperpla.htm&normal=gast_pix/normal54.htm
{kind=link}
{kind=link}
{kind=link}
Comments (6)
Anonymous said
at 12:01 pm on Dec 23, 2006
I added a pic entitled 'polyp classification'. Someone might want to add it to the presentation later...however, it has more than we really need. Got it from the website http://www.pathguy.com/lectures/guts.htm
Christine
Anonymous said
at 6:20 pm on Dec 25, 2006
we can remove our names from the individual categories before we turn it in. i just thought it would cut down on any confusion while it's still a work in progress. - iris
Anonymous said
at 9:57 pm on Jan 2, 2007
Hey I am done with my part. I may read it once more in the morning. Who is emailing the link to Dr. Brandon? I will not be able to because I will be at the dentist all afternoon tmrw.
Anonymous said
at 11:54 am on Jan 3, 2007
Iris, will you be able to send the link to Dr. Brandon? Just so there is no confusion as to who is sending it. Thanks for taking the lead on these projects. - Sinh
Anonymous said
at 1:18 pm on Jan 3, 2007
hey guys, the page looks great. nice job, everyone. soleil, if you haven't already sent the link to Dr. Brandon, could you cc all of us on the email?
thanks! - Iris
Anonymous said
at 3:13 pm on Jan 3, 2007
OK, I'll CC all of you in the e-mail to Dr. Brandon!-Soleil
You don't have permission to comment on this page.